THE EPIDEMIC OF YELLOW FEVER
IN NORFOLK AND PORTSMOUTH, VIRGINIA
DURING THE SUMMER AND FALL OF 1855.
By J. D. Bryant, M. D.
One of the Physicians of St. John's Orphan Asylum,
One of the Obstetricians of St. Joseph's Hospital, Phila., Etc., Etc.
Philadelphia: T. K. and P. G. Collins, Printers,
1856.(Courtesy of the Library of Congress)
[Page numbers in brackets.]NORFOLK and Portsmouth are situated on low plateaux, near the mouth of the Elizabeth River; Norfolk being on the east, and Portsmouth nearly opposite on the west bank. The immediate site of Norfolk is slightly more elevated than that of Portsmouth, though not sufficiently so to make it an exception to the general character of the neighborhood, which is low and marshy. Water lies near the surface of the ground, and may be obtained at a depth of from four to six feet, and in some places even less. Cellars and underground basements are consequently damp; and, when constructed, are unsuitable for the purposes of habitation. Portsmouth is intersected, or rather divided from Gosport, by a marshy space of about a quarter of a mile wide, and considerably more than that in length. The whole southern portion of the city faces upon this march. Across the eastern portion of it is a wooden causey, at present in a state of decay, connecting Gosport to Portsmouth. On the north side of Portsmouth is a run, or rather a narrow slip of marshy ground, which extends in a southerly direction through the city, with houses built upon its margin; the streets on each side being connected by wooden bridges. The muddy surfaces of both these marshes, with their vegetable growth, are, except for a short time during flood-tide, exposed to the rays of the sun, and emit a disagreeable odour. Besides these, innumerable marshy gulleys irregularly furrow the earth in a south and westerly direction. The surrounding country for many miles partakes of the low, damp condition of the immediate sites of the two cities. At [4] about eight miles south and west of them commences the Great Dismal Swamp, which extends thirty miles from north to south, and ten miles in width between Chesapeake Bay and Albemarle Sound. The soil is sandy, here and there somewhat loamy, and is of the modern tertiary formation. The natural vegetable growth, as might be supposed, is sparse and stunted, though the crops, suitable to the soil, are sufficiently generous. The population of Norfolk is estimated at 16,000, and that of Portsmouth at 11,000. Some of the streets of the former are well paved; and, considering the size of the two cities, houses of the better class and fine public buildings are numerous.
The condition of these cities during the summer of 1855 was particularly favourable to the prevalence of epidemic disease, and especially of yellow fever. Long continued observation has proved, that where animal and vegetable decomposition is extensively going on, in a humid atmosphere, with a temperature ranging from eighty to ninety degrees—three of the conditions necessary to the production of this disease—and when the fourth element, the miasm peculiar to yellow fever, is blended with their exhalations in sufficient quantity, it must prevail. The three first conditions existed to an unusual degree in Norfolk and Portsmouth, during the summer of 1855, and needed but the evolution or production of the fourth, to develop this disease.
As already stated, Portsmouth proper is bounded, on the south, by an extensive marsh. This is strewed over with logs, timber, wrecks of vessels, and other forms of vegetable matter, in every stage of decomposition; while the marsh itself, festering in the sun, generates offensive and noxious vapours. The same description, though to a much less degree; must be applied to the slip of marshy ground, which intersects the city north and south, as well as the others which intersect the various parts of the plateau upon which the city stands. But this is not all. Numerous docks on the eastern front of the city are, in like manner, so many points whence offensive and unhealthy gases are generated and wafted by every breeze over the neighbourhood. The dead level of the plain on which the city stands, and which, therefore, does not admit of adequate drainage, is another source of evil; since pools of water remain, for several days after every rain, in most of the streets, which are unpaved, while waste waters, compost, offal, or garbage of every kind, table and kitchen, animal and vegetable, lie where they are thrown, to putrefy under an almost vertical sun. This is particularly true of the lots attached to the houses, and the public streets in front of them. These sellæ familiaricæ are another source of offensive exhalation. These are seldom more than four or five feet deep; in many instances, no well whatever is dug, and the small sheds built up, simply indicate where the calls of nature are to be obeyed. Another eminent source of disease exists along the entire river front of the city, from the ferry to the navy-yard, in the shape of thickly set, ill ventilated, over-crowded, dilapidated frame tenements. [5] These, border immediately upon the offensive docks and the marsh, already named. They are occupied by the very poor, both black and white, two and three families being in each house, and, as an inevitable consequence, surrounded and choked up with filth of every description. Although the first cases of the fever occurred in persons from on board the Benjamin Franklin, at Gosport, where that vessel "broke out" her hold, yet it was in this portion of Portsmouth proper that the epidemic made its first and most deadly ravages. Not a human being of either sex or of any age, who remained within this precinct, so far as I could learn, escaped the fever; and most of them died. There was still another untoward condition of things found there. In consequence of the water lying so close to the surface of the ground, cellars and underground basements, as before remarked, are inadmissible. Nevertheless, they exist; and some of them were found, throughout the entire epidemic, to be tenanted by one, and even two families, and as it was poverty which kept them there, so, as may be supposed, its usual retinue of squalor and filth bore them constant company. But without dwelling longer in detail; such was the hygienic condition of Portsmouth when the epidemic commenced; and the wonder is, not that the pestilence prevailed, but that it has not annually swept the city from the time these conditions began to exist. And still more surprising is it that the city authorities should have suffered these evils to accumulate, in the full knowledge of the presence of the fell destroyer hovering about the Atlantic coast. Let us now inquire what was the condition of her sister city.
Norfolk, being the elder and more populous city, has a much greater number of citizens whose pecuniary means enables them to enjoy, to a fuller extent, the appliances of comfort and cleanliness. Its slightly increasing elevation of surface, as it recedes from the river, gives it also greater facilities of drainage. Many of its streets being paved, affords it another advantage in this respect, which Portsmouth does not possess. But, not-withstanding these favourable items in the account, her port-wardens and others give us ample information in regard to its unsatisfactory hygienic condition. On the 24th of July, about four days previous to the occurrence of the first case there of yellow fever, and one month after it had appeared in Portsmouth, we find the port-wardens advertising for contracts to cleanse some of the pestiferous nests, in the shape of docks, which threaten to be so many sources of malignant disease. In the same paper which contained these advertisements is an editorial, from which I make the following extract:
"We are glad to find that assiduous and well directed efforts are being made at last to place the city in a good sanitary condition, to clean out the gutters, remove the filth from the alleys and back lots, and thus to prevent the deadly and disastrous visit of fever or other infection, and perpetuate the good name which our city has justly acquired for salubrity. Roanoke dock, too, of which so great complaint has been made, is to be deepened, and the accumulated population, with its abominable stench, removed, as will be seen by the advertisement of the port-wardens. If this had been done two months ago, the public [6] would have been much better satisfied. But better late than never. (1) Extraordinary pains should now be taken, and continued, to get rid of all probably sources of disease. There are two or three other docks, both on the east and west of Roanoke Square, that are in a very bade state, and which also require immediate attention; and it is earnestly hoped the authorities will not be slow in using suitable means to correct all such exciting evils. The weather is sultry, humid, and unwholesome; vegetable and animal substances decompose and decay rapidly; and in some parts of the city there are very unpleasant and offensive odors, too plainly indicating the existence of filth that should not be allowed to remain an hour longer. Damp cellars and basement rooms should be examined, and filled up, or raised, and disinfectants freely applied." (2)
(1) These, and all similar works, should be performed only in the fall and winter months. The stirring up of such materials, or even of ordinary soil, in the spring, and especially summer months, has often been connected with outbursts of epidemic disease, and no doubt had its due share in the present case. How much more fatal must it have been when performed after the epidemic had already commenced!
(2) The Southern Argus, July 24th, 1855.
This account of the condition of Norfolk, made just anterior to the commencement of the epidemic, might, with equal truth and justice, be applied to the whole infected region covered by the two cities. The account has been drawn up from observation of the localities named, and by those who, for the sake of the character abroad of their fair city, might naturally desire not to display such facts, but yet who have not shrunk from the duty of making their sad plight publicly known, with the hope that the sanitary regulations, which the case so urgently demanded, might be made in time to prevent the sorrowful desolation which, three weeks later, swept like a hurricane through every house.To some it might seem unnecessary to seek further for the causes originating the late epidemic, than those which have been stated. At least three of the four conditions necessary to the production of epidemic yellow fever, existed there to an extent which justly excited the anxiety of the citizens and their city governments, viz: animal and vegetable matter decomposing in a humid atmosphere, with the thermometer ranging at 94 degrees in the shade. Remarkable for salubrity and healthfulness as Norfolk and Portsmouth are said to be, nevertheless yellow fever has several times appeared there, and in the former place it has frequently occurred since its advent in 1800; and on several occasions has made its first appearance in Barry's Row, where the first Norfolk cases occurred last summer. May not then, I ask, the peculiar poison, or whatever agent is supposed to constitute the fourth condition required to produce the disease, have been lurking amidst these elements, ready, when all the conditions necessary to its generation were constituted, to burst forth. Although the first cases of the fever of last summer did not originate in Norfolk, but in Gosport, the southern suburb of Portsmouth, nearly one mile distant from the former place, yet this is not impossible; and if it be a fact, as some say, that one case of the fever was treated at Gosport before any occurred on board of the Benjamin Franklin, then it becomes probable [7] that such may have been the origin of the late epidemic. And unless it can be satisfactorily proven, either that this was a mistake, or that the patient contracted the disease elsewhere, it would be extremely difficult to demonstrate that this was not the commencement of the epidemic. No case of the fever occurred at Norfolk until three weeks after it had appeared in Portsmouth; and when it did commence its ravages there, the first cases occurred in persons who had fled, panic-stricken, from Portsmouth. The supposition of its local origin, therefore, which I have advanced as a possibility, and, on the strength of the alleged case, as a probability, will not be acceptable to most minds. It is acceptable to mine only on the ground of that individual case being proven to be true. I am not satisfied that it is so proven. Nothing. so far as I can learn, was heard of it, nor was it even named until after the imprudence was committed of permitting a vessel, subsequently shown to be infected, to pass up from quarantine. Besides, the attending physician of the alleged first case, states it to have occurred on 24th of June; whereas, it was on the 17th of June that the first case actually occurred on board of the steamer. It remains, therefore, in the second place, to state the popular opinion respecting its origin; and by the term popular, I mean to designate not so much laymen as medical men. This opinion, then, as is almost universally the case, attributes the origin of the late epidemic to the arrival of an infected vessel from a foreign port. The scape-goat, in the present instance, is the steamer Benjamin Franklin, from the Island of St. Thomas. The history of the affair is as follows:—
The steamer Ben Franklin left the Island of St. Thomas towards the end of May, the yellow fever being at the time prevalent there. Driven by stress of weather from its course, it arrived at quarantine below Portsmouth on the 7th of June; having put into that port for repairs. "She was boarded by the health officer, to whom the captain stated that she had had no case of yellow fever on board; a fireman had died suddenly of disease of the heart, and the man who took his place had died suddenly of exhaustion; with these exceptions, the crew had been entirely free from disease. The steamer remained at quarantine twelve days, and no case of disease having occurred during that time, and the health-officer finding the vessel in a cleanly condition, with the consent of the Board of Health gave her a permit to pass up into the harbour on the 19th of June, upon the positive condition that the hold was not to be broken out. Having contracted with a party in Gosport to have her repairs done there, she was taken up to Page & Allen's ship yard (next to the Navy Yard). There she remained nineteen days, during which period, it is stated, the captain violated his engagement in having the hold broken out. On the 5th of July, a man who had been at work on board of her was taken sick, and his disease proved to be yellow fever. This case occurred twenty-eight days after the steamer's arrival. The patient died on the 8th of July, on the third day of his being attacked. The town councils of Portsmouth immediately convened, and issued an order to send her back to quarantine, which was done forthwith. Following this case were a number of others, among whom were six of the hands belonging to the steamer, who were sent to the U. S. Naval Hospital, where two of them died. In addition to these, twenty of the residents of Gosport contracted the disease, of whom five died; leaving fifteen cases under treatment on the 24th of July—making in all twenty-seven cases, and eight deaths, in the space of nineteen days. At this date the disease was confined entirely to the vicinity of Page & Allen's ship yard, which was boarded up, and all communication with it interdicted." No case is shown to have existed beyond this small infected district which was not contracted within it; and Norfolk, as yet, remained entirely free from every trace of the disease.
This, however, is not the whole of the story. Deception had been practiced upon the health-officer; for, on the day following that on which the steamer arrived at Gosport (June 21), and fourteen days before the first case of any citizen of Gosport occurred, a seaman, named James Palmer, had been received from her at the U. S. Naval Hospital. In half an hour afterwards, he was visited by the surgeon of the hospital, who found him moribund, but perfectly rational. The man stated that he was taken sick on the 17th—two days before leaving quarantine. Before 12 o'clock P. M. of the day he was taken to the hospital (21st), this seaman died of black vomit. (1) It is thus rendered evident that deception had been practiced upon the health-0fficer, and that the first case of the yellow fever was that of a seaman belonging to and on board of the Benjamin Franklin. The authorities immediately communicated these facts to the owner in New York, who promptly dismissed Bynam from the command of the vessel, and appointed Captain Harrison to succeed him
(1) The case of Mrs. Fox, above alluded to, occurred on the 24th of June, seven days after that of James Palmer, and three days after his death. The date in the former case is given on the authority of her attending physician; that of the latter, on the authority of the Norfolk and Portsmouth Herald of July 26, 1855.
Although the panic had commenced, yet, up to the 24th of July, no case of the fever had originate out of Gosport; but, from this date, it commenced its ravages along the eastern edge of the city, among the squalid poor residing in the dilapidated tenements bordering upon the marsh already referred to, and along the river front. It swept through these like a tempest, sparing none, and slaying three in every five. The panic was now complete. The fell destroyer could not be arrested by barricades, or hygienic measures applied too late, and held high revelry over its prostrate victims. All, who could, fled. But, vain expedient! they carried the seeds of pestilence within them, and many fell by the way. The ties of blood were sundered; bonds of alliance were as if they had not been; friend shuddered, and shrank from friend; the sick and dying lay in hopeless despair, with none to moisten their parched lips, nor administer a soothing draught; while burial for the dead was with difficulty obtained. Though a departure from the cold formulæ of [9] the statistician, this is no fancy sketch; it falls far below the truth. The population of the flourishing and heretofore healthy town of Portsmouth was reduced by flight or death from eleven to four thousand, and that of Norfolk from sixteen to five thousand. Except a few brave hearts, which nothing could appall, all who were not forced either by sickness or other necessity, to remain, had now left. The stores were closed—not even excepting the drug shops—their owners having, like the rest, either fallen or fled. The markets were unattended; none being willing to approach the city to supply its wants. And had it not been for the benevolence of other cities, gaunt famine must soon have added its horrors to those of the pestilence. There was not one house in which there were not some dead, until, as near as can now be ascertained, forty-five per cent. of the population died. Of the resident physicians, only four survived. The coloured people resisted the epidemic influence better than the whites; and I believe I may hazard the observation, that their degree of resistance was in proportion to the admixture of white blood. The mortality among the whites at Portsmouth is stated to be 42-1/3 per cent., while that of the blacks was only 5-1/4 per cent. The pure African resisted better than the mulatto; and the degree of resistance in these again was less and less according to whether they were half-breeds, quadroons, or still nearer approximating to white. I made this subject a point of special observation, and my only reason for qualifying it is, that the impression is derived but from one series of observations. Others, of more enlarged experience, may now or hereafter be able to say whether or not it be correct.It is on the 31st of July that we find the first public admission that the epidemic had invaded Norfolk. The announcement was made in these words:—
"Every part of our city, excepting (we regret to state), Barry's Row, is healthful, and free from all epidemic diseases. In the buildings alluded to, situated near the southern terminus of Church Street, there have recently been seventeen cases of malignant fever. There have been four deaths; six have nearly recovered, and seven are said to be exceeding ill. We were as much surprised as others to hear this statement (yesterday) from a reliable source. But really it is no great cause of wonder that an infectious disease should break out in those abominably filthy hovels, in which there have been crowded during the intensely hot weather of the present month, a large number of extremely indigent persons, who had not the means, if they had the desire, to observe any degree of cleanliness. Sweltering amid the most disgusting filth inside of the houses, and just without the back doors, it is remarkable that the miserable and unfortunate inmates have not sickened and died by the dozen long ago. But, as if to hasten and insure the production of pestilence, at this ill-fated locality, several families of a congenial stamp removed over and took lodgings in that horrible and sickening receptacle of the destitute and suffering. The Board of Health have ordered the immediate removal of the sick and their families to Oak Grove, some distance beyond the city limits. The occupants who were not sick will be removed forthwith, and the street above and below the Row has been barricaded." (1)
(1) The Southern Argus, July 31, 1855.
Such is the first public acknowledgment of the commencement of the epi- [10] demic in Norfolk. But it is believed to have been present there, unknown to the respectable editor whose words I have quoted, at least two weeks previous to the date of its public announcement. This is not only implied by another article in the same paper, which speaks of the noble zeal and commendable promptness with which the Sisters of Charity had devoted themselves to the task of nursing the victims, but also by the article itself, which speaks of seventeen cases; of four deaths as having occurred; and of six patients as having nearly recovered; all of which, in view of the course of the disease, could not have taken place under a fortnight. Considerable anxiety seems to have been exhibited to conceal the presence of the disease at Norfolk; and, with the data in hand, it is not easy either to affix the precise date of the first case there, or to state whether it was imported from Portsmouth, or originated in Barry's Row. It was, however, only on this day, July 31, that the Board of Health of Norfolk issued its first daily bulletin. (1)
1) OFFICE OF THE BOARD OF HEALTH, July 31, 1855.—Report for the twenty-four hours ending this day at 12 M.: Cases of fever—6. Deaths—none.
The above are exclusively in Barry's Row. The Board having nothing to report from any other part ofthe city.—T. G. BROUGHTON, Secretary.
From these evidences, therefore, we may fairly consider the epidemic as having a firm hold upon both cities at this date. Popular opinion, as already stated, attributes the origin of the epidemic at Gosport to the steamer Benjamin Franklin. But whether it was from this same source conveyed to Norfolk, will, I suppose, ever remain a disputed point. That yellow fever patients were imported, or rather transported themselves, from Gosport to Norfolk, simultaneously with its appearance in the latter place, is certain. In fact, every case which occurred there, at the commencement of the epidemic (already spoken of in connection with Barry's Row), is clearly traced to Gosport—every case, except the first case, which was that of a patient who died in a densely settled neighbourhood on Main Street, at the precise locality where the epidemic of 1821 commenced, and where several sporadic attacks, since that time, have taken their start. Unless, therefore, it can be shown that this patient had visited and become tainted in the infected district at Gosport, there is no evidence but that this epidemic may have commenced, as have several previous spells of the disease. There may not, however, be any necessity for this refinement of analysis. East and West Philadelphia, New York and Brooklyn, are not more intimately related, as to position and intercourse, than Norfolk and Portsmouth, and every serious epidemic which prevails in the one, must, in the natural course of things, affect the other. In treating of the origin, therefore, of this epidemic, while it cannot be denied that grave suspicion rests upon the steamer Benjamin Franklin, it should not be forgotten that the yellow fever has frequently presented itself in that region since the year 1800. Whatever inference is to be drawn from the alleged facts, I leave [11] to others. If they do not seem clear and satisfactory, it is from the nature of the facts themselves. They are stated as they occurred. One thing, however, may be regarded as certain, namely, that unless all the conditions necessary for the production of epidemic disease had been ripe for action, there would have been no epidemic last summer in either place, even though the entire crew of the Benjamin Franklin had been infected with it. The poison of yellow fever existed, last summer, at Savannah, at Charleston, and elsewhere; yet there was no epidemic of the disease at either of those places. Fugitives carried it from the very heart of the infected district of Virginia to Baltimore, Philadelphia, and New York, and yet no epidemic disease whatever arose in any of those places; while, on the other hand, the disease may, and in all probability would have existed epidemically at Norfolk and Portsmouth, even if the Benjamin Franklin had never entered that port. Nevertheless, without the fear of being considered a contagionist, (1) I must hazard one other observation, indicative of the extreme danger and criminality of permitting infected vessels, at certain seasons, to pass up to the wharves of our cities and towns. The atmosphere, miasm, gas, or whatever other name may be used to designate the pestiferous contents of such a vessel, is deadly, as is abundantly proved in the history of almost every epidemic. Scarcely one occurs, which is not by popular rumour, or medical, or judicial decision, connected with the arrival of one vessel from an infected port; and as no city can guarantee the absence of those conditions which correspond with any given malignant agent, it would be as insane to permit their unmolested approach, as it would be to transport a Barry's Row to the same place. We know as little about the nature of the epidemic influence, as we know about the law which starts it on its mission—as the cholera—around the world, or keeps it confined—as the yellow fever—within certain zones or parallels of latitude. And as to the particular type of this latter disease, which has now three times, in as many consecutive years, raised such a wail of woe throughout our land, may it not be that its giant footsteps directed by no law with which we are acquainted, are, in spite of all our puny efforts, unerringly directed northward? We have seen its fearful, almost unprecedented ravages at New Orleans, in 1853. We next see it at Savannah and Charleston, in 1854; and now, in 1855, in Norfolk and Portsmouth. Baltimore, Philadelphia, and New York like directly in its present course.
(1) The connection of vessels arriving from infected ports with the origin of yellow fever, does not, as it is charged, necessarily involve the idea of contagion. The exhalations of bilge-water, and the otherwise infected air of such vessels, may be the identical agent which, blended with the morbific elements on shore, combine to constitute the precise conditions upon which the evolution of the disease depends. That vessels are and have been, from the earliest periods of which we have any accounts, connected with the rise of epidemics, the public voice and the best medical authority constantly attest.
I have ventured upon these observations, in the full knowledge of the fact [12] that yellow fever does not, like Asiatic cholera, pursue a direct migratory course. But the time was when cholera did not; and when we consider that a peculiarly malignant type of yellow fever is ravaging our seaboard, whose present course is northward, there is reason to fear that it may have sufficient force to make as deadly an impression here as it has elsewhere. When, in 1853, one hundred and seventy cases could occur in Philadelphia, of which one hundred and twenty-eight died, no apology need be made for raising a warning voice in time for sanitary reform.From the 27th of July, the ravages of the pestilence steadily increased, especially at Portsmouth; and three week after this date, its violence, or rather the number of cases at Norfolk, greatly exceeded those of the former place, Norfolk being the more populous city. By the 25gh of August, the average number constantly sick in Norfolk was five hundred, the population then being estimated at five thousand. The number of deaths were from sixteen to twenty per day, and the new cases exceeded twice that amount. In Portsmouth, at the same date, the whole number of sick was about four hundred, in a population estimated at four and a half thousand. The deaths averaged seventeen, and the new cases about thirty per day. The epidemic reached its height, at Portsmouth, by the 10th of September, on which day the reported number of deaths was thirty-one. At Norfolk, it attained its maximum about the 22d of the same month, on which day the number of deaths was twenty-four. On several days, the deaths much exceeded both these figures. These statements are made on the authority of the published reports of the sanitary committees of both places respectively; but they fall much below the actual facts. The returns of the physicians were very irregularly made, and sometimes omitted entirely; while the published lists were frequently made from information derived from other sources than the official accounts. It is also well known that numbers sickened and died in both places, without the cognizance of committees, or any medical attendance whatever. The estimates here presented being derived from actual lists, containing the names and ages of the victims, are at least not chargeable with being exaggerations. In reference to this subject, a respectable publicist of Norfolk says:—
"The vast majority of the victims were buried as 'unknown.' Could the entire number of those who died at home and abroad be ascertained, it would sum up fully 2,000. The records of Mr. Hawkins, at the almshouse, show that 1,200 were buried in two grave-yards under his charge, viz: the Cedar Grove and Elmwood cemeteries: 800 would, we think, be a moderate estimate for the burials in other places in and out of the city. We always found, when we undertook to 'inquire out' the number of deaths on any given day, that it invariably exceeded the most extravagant guesses."
The estimate given above probably falls short of the actual number; but taking it as the basis, and adding to it the estimate made of the entire mortality of Portsmouth, which is about eleven hundred, and we shall have the fearful mortality of three thousand one hundred in a united population of [13] nine thousand; or, in other words, a mortality of thirty-five per cent. of the whole, and upwards of forty-three per cent. of those attacked. [These two figures are transposed in ink on this page, so the sentence would read . . . a mortality of 43% of the whole, and upwards of 35% of those attacked.] (1)
The climate of Norfolk and Portsmouth is bland and agreeable, and generally exempt from extremes of heat and cold. It is somewhat damp, and during 1855 exceeded, in this particular, the average of ordinary years. The temperature of the season was also higher than ordinary. The following table for which I am indebted to the politeness of Dr. L. W. Minor; of the U. S. Naval Hospital, Portsmouth, exhibits the maximum, minimum, and mean ranges of the thermometer for each month respectively, during which the pestilence prevailed. The first case occurred June 17, the last at the close of October, including a period of 137 days:—Some of the changes of temperature were very sudden, and often accompanied by rain. This was especially true of September, when fires, though seldom kindled, were comfortable, and indeed necessary to modify the dampness and chilliness of the atmosphere. Overcoats and cloaks were comfortably worn during these spells of bad weather, and as quickly thrown aside, a day [14] or two afterwards, on the reoccurrence of sunshine. These changes always augmented the number of new cases and greatly increased the mortality. Those who had hitherto escaped from attack, and seemed boastfully to calculate on entire immunity, were at such times seized upon, and suddenly hurried to the grave. In numerous instances, also, the disease ran its course more rapidly than at an earlier period.
The symptoms observable in this epidemic did not vary, except perhaps in their intensity, from those of ordinary cases of the same disease. A sense of weariness, accompanied with lassitude or languor of body or mind, restlessness, heaviness, and depression of spirits, generally ushered in an attack. Most commonly those were attended with fugitive, or even continued pain in the head, back, joints, and limbs. When in the head, it sometimes seemed intensely concentrated above the supra-orbital ridge; at others it was more diffused through the whole frontal region. The knees would suddenly give way, as if the patient were unexpectedly struck from behind. This was my own case; and I should have fallen had it not been for an object near me, which served as a support. The pain in the back was often more persistent and severe than some of these symptoms, and would not unfrequently continue throughout the whole course of the disease. A creeping sensation, or perhaps a positive chill, with shivering, or more rarely an actual ague fit, would announce its approach, together with loss of appetite and a disagreeable bilious taste in the mouth. These symptoms, so far as I observed, were not generally of long duration, anterior to the full development of the attack. Tenderness of the epigastrium generally accompanied its inroads, and was sometimes increased to a degree of soreness that would not bear the slightest pressure, not even of dress, or the bedclothes. It was usually attended with nausea, eructations, or vomiting. In many cases, the remedies given to arrest this, increased its tendency; they seeming to act upon the tender and inflamed viscus as any other foreign substance, to be ejected as soon as swallowed. In other cases, again, these phenomena did not occur for several hours, or even days, after the commencement of the attack. When the fever was fully established, the face—especially the upper part of it—became flushed, the eyes injected, and, in a few cases, early tinged with yellow. The pulse was characterized by want of vigour and energy; it was easily compressible, and sometimes would entirely disappear under very moderate pressure. It was generally accelerated, rising to one hundred and twenty or thirty. It rarely fell beneath its normal rate at the outset, but afterwards fell to sixty, or even fifty beats per minute. In one instance which fell under my notice, it went down to forty-two. The skin was hot and dry; the mouth and fauces were generally moist, though in some rare instances they were also dry; but, in either case, the thirst was nearly always insatiable. The respiration was hurried, as if the patient were overcome by rapid walking. In most instances, the tongue was uniformly coated white; in others, this was blended with a bilious coating. Flatulency was a marked [15] feature in some cases. The bowels were generally constipated, though in no case which fell under my notice, obstinately so. The appearance of the feces was dark bilious, bronze, or black, extremely offensive, and, after the first discharge or two, small in quantity. The urine was also scanty, though not always deep coloured. Great restlessness and anxiety prevailed in almost every case—increased, in many, to uncontrollable fear and dread. These emotions were uniformly depicted with greater or less intensity on the countenance. Delirium sometimes supervened on the formative stage, but more frequently stupor, with a distressful or apprehensive look.
I have confined this account of the symptomatology of the first stage to the points which fell under my own immediate notice. There may have been other symptoms equally well marked, in individual cases, but I think the above will serve to show with sufficient exactness the general aspect of the onset of the disease in this epidemic. Some of those here mentioned would run through every stage, and end only with the termination of the case; whilst others would subside in from ten or twenty to seventy hours, modified, or enduring with variable intensity, according to the idiosyncrasy of the patient, or the nature of any chronic affection with which he may have been previously afflicted, or to his moral habits—generally proving fatal to those addicted to intemperance, excessive venery, masturbation, and the like. Those debilitated by the latter were especially obnoxious to their force; and of the intemperate, but few escaped, and still fewer survived an attack.
After the symptoms above described had continued from one to three, or perhaps even five days, they took one of two directions; either they subsided, and the patient advanced happily onward to convalescence and ultimate health, or they increased in severity and terminated in death. The intermediate or secondary stage, so precisely defined by some writers as the stage of abatement preparatory to a fresh and more deadly development of the disease, did not form a very distinctive mark in any case which fell under my notice. There were patients who, after the subsidence of the first paroxysm, seemed destined to be restored to health, and who relapsed and died. But their relapse could be traced to adequate causes, and they in no sense seemed to be passing regularly through uniform, successive stages of formation, abatement, and collapse. Unless for recovery, the disease did not visibly relax its hold until it laid its victim low. The subsidence of the paroxysm, therefore, was generally a favourable prognostic. When the primary attack pursued a favourable course, the fever subsided in from three to five days—rarely so early as the second day, though cases even of this are not wanting. The skin became soft and moist, or was bathed in a profuse perspiration; the flushed face and injected conjunctiva resumed their natural appearance; the desire for cooling drinks passed away; the accelerated pulse was retarded, and became rather more firm; the headache, pain in the back, and other distressing symptoms, all disappeared. The mind awoke from its torpor; anxiety gave place to a more cheerful and hopeful condition, and the [16] patient was dismissed cured in from ten to fifteen days. In mild cases it might be somewhat earlier, while in very severe cases it might be protracted to one or more weeks beyond this period.
But when the course of the disease was not favourable, and the case ran on to the collapsed state; then, all the symptoms above described became alarmingly exaggerated. Extreme weakness and utter prostration ensued; the pulse became quicker, irregular, and still more easily compressible; the blood ceased to move in the capillaries; petechial spots here and there empurpled the skin, or expanded, in the dependent parts of the body and the extremities, to broad patches, resembling somewhat the vibices of purpura hæmorrhagica; in some severe cases, the vital fluid would burst its lax and feeble barriers, and stain the surface, especially in the parts lined by the mucous membrane. The meatus of the ear, the nasal passages, the gums and other parts of the mouth, the throat, stomach, bowels, kidneys, urinary passages, rectum, and vagina, were all the seats of more or less excessive discharges of blood. In one case that I witnessed, the hemorrhage from the bowels resembled a flooding from the uncontracted uterus, and continued to flow in a copious stream for more than an hour after death. In another case, that of a youth, who came under my own care, hemorrhage of the throat, mouth, and nostrils, persisted daily for more than three weeks, and did not entirely subside until after convalescence was fully established. This was a desperate case, and further remarkable for the thick, dry, almost black coating of the tongue, which was intersected with deep fissures, through which the blood unremittingly oozed. The teeth and bleeding gums were covered with sordes, emitting with every expiration the most offensive odor. After the fifth day, the yellow hue, if present, deepened, and overspread the face, extremities, various parts of, or the entire body. Many cases, however, had no tinge of yellow whatever during the whole course of the disease, unless it terminated fatally, when it invariably suffused the entire body. It varied from the ordinary pale bilious hue to the deepest jaundice; in shade not always clear and bright, but as often tawny or dusky. Though the yellow hue of the skin always indicated severity of attack, it could not be regarded as a fatal symptom. (1) The urine, always scanty, varied in colour from a deep orange to dark brown; while the feces took on every shade, from the ordinary bilious stool to the deepest black, often presenting the appearance of tar, and always extremely offensive. Tenderness of the epigastrium, though frequent and intense, was often less prominent than gastric irritability. In the case of one patient, who died of black vomit, very considerable pressure upon the epigastrium was made by me without exciting the least complaint; and yet, everything swallowed by him was instantly ejected.
(1) Dr. Warren, in his treatise of the fever at Barbadoes, attributes the discoloration of the skin not to "a suffusion of bile, but rather to a colliquation, and perhaps a gangrenous diathesis of the sanguineous mass, occasioned by the force of the deleterious venom that had been infused into it.
[17] Emesis was frequently unattended by black vomit; but its tendency was to that effect. When this did occur, it usually began with the contents of the stomach slightly clouded; in an hour or two a light brown flocculent matter would appear; this would deepen in colour until the fluid emitted assumed the appearance of weak coffee, and contained brown flakes. This again, if the patient survived long enough, thickened and became still darker, and at last almost of inky blackness. It had a peculiar odour, scarcely describable, but once perceived, never forgotten. A similar odour was sometimes exhaled from the skin in patients without black vomit. Various ineffectual attempts have been made to describe it. Dr. Rush says it resembles the washings of a gun; and he again likens it to the smell of liver of sulphur. Dr. Rochoux regards it as analogous to gangrene. These, and all other similitudes, are but approximations. The odour is sui generis; and when a proper name is found for the disease, and applied to it as a prefix, it may be correctly indicated, but it can never be described. Patients having black vomit died in from three to twelve hours after it was fully established. In malignant cases, it often immediately followed the onset of the attack, and the patient would succumb on the third, fifth, or at most seventh day. A few, gifted with extraordinary animal force and mental courage, might protract the struggle a little longer than this, and then yield. Apathy, which characterized the primary attack, soon increased; and the attention, which before might be temporarily excited, totally failed. The patient lay with closed eyes, lethargic, or even comatose. The heart now almost ceased to throb, and the pulse was arrested by the slightest touch. Respiration was slow and laborious; or, in others, hurried, occasionally interrupted by hiccough, sighing, and, if the power and material remained, black vomit. But most commonly, at this stage, the bowels gave way, and frequent discharges of a dark, tarry matter took place, the skin became cold and clammy, and in some cases exhaled the disagreeable odour referred to above; at times it became moist, and the hands and feet shriveled. While the symptoms of the third stage progressed, some of the patients would exhibit every degree of mental aberration, from the mildest form of delirium to the most uncontrollable, maniacal violence. Thus, while one would lie in passive stupor, with occasional mutterings, and breathe his life out in awful calmness, another would defy the united strength of several to control his motions, or require to be firmly strapped to his bed, while the neighbourhood would resound with his fearful shrieks, until collapse ensued, when his last breath, and the last wave of the life current would fitfully subside, and naught but the saffron corpse remain.None of the symptoms, so far noted in this account, essentially, per se, predicated death. Patients who have suffered them singly and combined survive, and now enjoy their accustomed health. They were, of course, the exception, not the rule. The ratio of mortality from them varied considerably. For example: I know of but four cases having black vomit which recovered, out of five hundred patients, in whom this phenomenon was pre- [18] sent—less than one per cent. A very remarkable case of recovery after black vomit was that of a seaman, who was admitted into the United States Naval Hospital, near Portsmouth. This man was under the care of Dr. Randolph Harrison, (1) who has kindly furnished me with the following particulars: "On the third day of his attack, black vomit made its appearance, and lasted three days. After an absence of two days it again returned, lasting about thirty-six hours; then, after a very dubious existence of a week, he began rapidly to amend. His convalescence continued for eight or nine days, when, from a slight bruise received in the night, the whole forearm became inflamed, pus formed, and the tumour was lanced in five places. The drain from this reduced him to a very precarious state, through which he was carried by stimulants, tonics, and a generous diet. His treatment, during the continuance of the vomit, and for some days after, consisted of large doses of plumbi acetas, by the mouth, and by enemeta; milk, ad libitum, and soup enemata." The ratio of recovery from the collapsed state somewhat exceeded this, it being, so far as my observation extends, about five or six per cent. I have heard it stated at twelve or fifteen per cent.; but such is not my experience in relation to it.
(1) Dr. R. Harrison had just mailed his letter of resignation as surgeon in the U. S. Navy, when he received orders from the department to repair to the Naval Hospital, in the yellow fever district. He nobly withdrew his resignation, repaired to the post of danger and of honour, and remained on duty throughout the entire epidemic.
There was one symptom from which death could be invariably prognosticated, viz: suppression of urine. It was a certain indication of the general dissolution or breaking up of the animal functions. Perhaps not one patient, certainly not more than one, in whom it occurred, survived. The ratio of cases exhibiting this symptom did not probably exceed ten per cent. It occurred chiefly in the third stage of the disease; and, excepting one case at the Naval Hospital, who survived three days, every patient died within forty-eight hours after the suppression commenced. In every instance, the catheter, when withdrawn, was devoid of the urinous odour, and its punctures were clogged with mucus. Estimating the whole number of deaths at four thousand, and the ratio at ten per cent., the case of recovery above alluded to is one out of four hundred. Dr. Pennell, as quoted by Dr. La Roche, mentions a similar case. He says, "out of many hundreds of patients whom he treated, during the epidemic at Rio Janeiro in 1850, he remembers but one instance of recovery in patients with suppression." This is the more remarkable in view of the large proportion of cases in which this phenomenon occurred, which he states to be eighty per cent. of all the fatal cases. Dr. Wragg informs us of fifteen patients whom he treated, having suppression in the first stage of the disease. The suppression persisted for three days, when twelve of the patients died, and three recovered. This remarkable statement is made, it should be remembered, respecting cases in which the suppression occurred in the first stage of the disease, when the pa- [19] tients may be supposed to have been less wasted and broken down by its ravages. Even with these remarkable exceptions, however, suppression of urine still remains the most certain symptom of dissolution; and when it occurs in the final stage, and continues for thirty-six hours, it is the inevitable precursor of that event.The treatment of patients in this epidemic was as varied and opposite as the localities from which the different practitioners came. Each proceeded upon that plan, which either had obtained at home, or may have been derived from his own preconceived ideas. But after a few days' experience, and by comparing notes, it finally settled down into some degree of uniformity. The means most in vogue, and which seemed to produce the most favourable results, did not vary from those which obtain in the ordinary epidemics on record. There was, however, one exception to this general remark, viz: venesection. This was universally discarded. A physician who arrived at the infected district, well supplied with lancets, said to me: "When I approached the bedside of my first patient, lancet in hand, I looked, I trembled, and replaced my lancet in its case; nor did I see one patient after this from whom I would have dared to draw blood." Dry cups, however, were sometimes used to overcome local congestion.
The first remedy almost invariably administered, in the first stage, was a brisk cathartic. This generally consisted of ten grains of the mild chloride of mercury, combined with six or eight grains of jalap or rhubarb; followed, in from five to seven hours, with an ounce of the sulphate of magnesia, or castor oil. The oil was preferred by many physicians; but, in my own practice, the saline cathartic, sometimes combined with senna or magnesia, seemed to act more happily. They were more easily retained, while their refrigerating effects aided in breaking the fever in its formative stage. It occasionally happened, as for example in plethoric patients, when there was absence of nausea, gastric irritability, or but little tenderness of the epigastrium, and when the stomach was charged with ingesta, that an emetic of ipecacuanha most happily preceded the administration of the cathartic. When this could be resorted to, it of course greatly expedited the main object, which was to empty the primæ viæ as quickly as possible, preparatory to the exhibition of the sulphate of quinia, and to hasten the mercurial impression. These remedies were, in the opinion of some, the sheet-anchor of hope. In slight cases or irritability of stomach, mustard poultices to the epigastrium, with the internal use of the effervescing draught, would generally be sufficient to allay nausea and distress. But in more severe cases, a fly blister, and the denuded surface sprinkled with the eighth or quarter of a grain of acetate of morphia, would be demanded to effect the desired object. It is needless to remark, however, that numerous cases would defy all attempts to bring them successfully under the healthful control of remedial measures. Supposing the means just indicated to have been effectual, the following treatment seemed to have very favorable results: One or two grain doses of calomel every hour, with [20] or without opium, were administered until its constitutional effects appeared. Salivation being attained—and it was so in three out of five cases—was continued throughout the entire course of the disease. It may be here noted, that while, on the one hand, it was not so difficult to salivate as is stated by some writers, on the other, the assertion that patients, who are salivated in the early stage almost always recover, did not seem to hold good in this epidemic. So little, indeed, was salivation relied upon by some practitioners, that they seldom attempted it; and in the United States Naval Hospital it was, if not entirely discarded, at least of but little repute; while the mercurial plan generally was not held in much greater esteem. Simultaneously with the measures just noted, mustard pediluvia, and mustard poultices to the extremities, were freely used, and often with the most happy effects, so far as relief of the oppressed vital organs was concerned. Many cases occurred, in which the results from these remedies were so salutary as to excite the wish to try the effects of mustard baths in the private houses, precluded a fair trial of their efficacy. I feel well persuaded that some valuable lives might have been saved by this means. In many cases, the capillary circulation was so timely restored, and the vital functions relieved, that the patients were enabled to sustain the terrible shock of subsequent paroxysms, and eventually recover. In connection with these stimulating remedies, the Dover's powder was successfully used, where cerebral congestion did not contraindicate it. Ice, iced water, iced tea, lemonade, and other cooling drinks, were always refreshing, and administered with advantage whenever they could be obtained. Sometimes, in spite of advice to the contrary, they were taken in extravagant quantities, and by persons who should not, perhaps, have taken them at all, thereby depressing the tone of the stomach. Several deaths occurred, which were certainly hastened, if not wholly attributive, to excess in this particular. Hemorrhage was happily met and arrested by acetate of lead, administered in two-grain doses every hour or two hours. I have in this way administered sixty or seventy grains with the desired result, and wholly unattended by any bad symptoms. It is also beneficially employed in the way of enemata, and as a gargle and mouth-wash. Creasote and nitrate of silver were effectually employed for the same purpose. If these remedies, and others of a like nature, succeeded, and the first paroxysm subsided, the next step was to nourish and support the system by suitable stimulants and diet. Weak animal broths, eggs, milk, milk and water, milk and lime-water, and farinaceous articles, formed the chief staples of diet; while wine sangaree, bark, carbonate of ammonia, and other tonics, were all employed, in various degrees and modes, to meet the indications arising, and to suit the views of the respective practitioners. But if the disease, instead of abating, as here supposed, multiplied its terrors by taking on the more fearful symptoms of the third stage, extreme weakness, utter prostration, black vomit, hemorrhage, diarrhœa, subsidence of cardiac action, stagnation of capillary circulation, [21] appearance of petechia, cold clammy skin, apathy and collapse—then it became the medical attendant assiduously to linger by the bedside of his patient and redouble his exertions. Increased doses, and in stronger form, of all the ordinary tonics, with wine, brandy, milk punch, and strong animal broths, were then demanded and freely used. When irritability of stomach forbade their administration in the ordinary way, they were given by enemata. Many owe their restoration to health from these desperate circumstances to such assiduous care.
Sulphate of quinia was the most prominent remedy which obtained in the treatment of this disease; the remedy par excellence, upon which the physician's hope of success most depended. It was regarded by many as a specific remedy, and was accordingly exhibited in every mode—by mouth, by enemeta, and by inunction; and in every degree, from one to one hundred grains. A certain practitioner was accustomed, in certain cases, to repeat a forty grain dose within the twenty-four hours, according to his own statement with favourable results. His professional brethren were not disposed to praise nor imitate his heroism. Quinia, in large doses, has occasionally been effectual in diminishing the frequency of the pulse, and hence has been regarded by some as a sedative. It certainly had this effect in many instances during the late epidemic. Administered in twenty and twenty-five grain doses during the most intense febrile action, it is asserted to have immediately broken down the attack in its first paroxysm. It has also been not less effectual in arousing the torpid energies, when, in the last stage, no other remedy availed. The ordinary exhibition, however, of this medicine was as a tonic, in one or two grain doses every hour or two, or in three and five grain doses, at like intervals, until twenty or thirty grains had been taken. Thus administered, it certainly exceeded in efficacy all the other tonics combined. But though its beneficial results in this, as in every other form of miasmatic fever, is sufficiently demonstrated, I am not prepared to admit, much less affirm, that quinia, or any other known remedy, is a specific cure for yellow fever. (1)
(1) Compare the latest records of epidemic yellow fever, in which quinia is brought to bear upon the disease in every conceivable mode and measure, with the earliest reliable accounts we have on the subject, and the ratio of mortality will be found to be as great now as formerly. In the epidemic at Philadelphia, 1699, the mortality was 220 in 3,800, about 6 per cent.; in that of 1793, it was 4,044, in a population of 50,000, about 10 per cent. These were before quinia was brought to bear upon the disease. In Norfolk and Portsmouth, in 1855, with all the advantages of experience and new remedial agents, the mortality, putting it at the lowest estimate, was 3,077, in a combined population of 9,000, about 34-1/2 per cent. These are not isolated cases; other tables exhibit similar results. Why is this, if quinia be a specific cure for yellow fever?
It may serve the purpose of clearer elucidation to display several distinct cases, together with their treatment. The cases presented are of every grade. [22] They have been selected as heads, or representatives of classes, and will, therefore, serve to show, with considerable accuracy, the general aspect of the entire epidemic.CASE I.—Mrs. McB—, aged 23 years; a native of Ireland; had resided at Portsmouth one year. Saw her within four hours after the development of the attack. Had considerable fever, irritable stomach, slight nausea, no tenderness of epigastrium, pain in the back and anterior part of the head very severe; upper part of the face flushed, conjunctiva but little injected, tongue coated white; pulse 100, rather firmer than usual; a sickening fetid odour suffused the bed and its neighbourhood. This is the only case in which the fetid odour was unmistakable so early in the disease. Ordered mild chloride of mercury, grs. x; jalapa, grs. v; to be followed, in six hours, by castor oil, see; mustard bath to feet and legs; permitted cooling applications to head, and small draughts of ice-water, if much desired.
2d day. Febrile symptoms subsiding; pulse 94; pain in head and back relieved, but still present; stomach quiet. Ordered mild chloride of mercury, grs. xv; Dover's pul. grs viij; divided into twelve parts; one every hour. Repeated mustard pediluvia.
3d day. Febrile symptoms subsiding; pulse 88, but soft, and easily compressible; patient complains of being weak, no evacuation of bowels during last twenty-four hours. Ordered castor oil see; and, after its operation, gave sulphate of quinia in one-grain doses every two hours, until twelve grains were taken.
4th day. Patient salivated; fever subsided; skin soft and moist; pulse 80, and more firm; slight pain in back, none in head. Continued sulphate of quinia as before; allowed chicken broth.
5th day. Conjunctiva slightly tinged with yellow; all the other symptoms abated; patient cannot see how it is that she should feel so weak in so short a time. Continued sulphate of quinia and chicken broth, and allowed tea and toast with a soft-boiled egg.
6th day. Bowels constipated. Ordered a moderate purge of sulphate of magnesia.
7th and 8th days. Convalescent. No further treatment.
9th day. Patient dismissed well, with some general dietetic rules. This case is presented as a specimen of the simplest form of the disease. It is, with slight variations, the type of a large proportion, probably one-fourth of all the cases which occurred. It is proper further to remark, that the patient passed through it more favourably than many who were less severely attacked, in consequence of her admirable composure. She was perfectly placid, and free from perturbation. It not unfrequently happened that, while one patient, having but an ordinary attack, would, through worriment and the depressing influence of fear, bring on fatal symptoms and die, another, even more severely handled, who could overcome his anxiety, would readily recover. And I [23] think it was here made sufficiently evident that perfect calmness and composure are more valuable coadjutors towards a favourable termination of a case than four-fifths of the pharmaceutical remedies in vogue. This was fairly illustrated, in a general way, during the height of the epidemic. The medical corps of Portsmouth had dwindled down to four or five in number; all the drug shops were closed, and but little food could be obtained. Through the force of these circumstances the people were panic-stricken, and thus fell trembling victims to the destroyer, dying, as it might be said, from fright. So soon as the medical corps was reinforced, and nurses, and medicine, and food were resupplied, hope and confidence were comparatively restored; and, though all continued obnoxious to the epidemic influence, the ratio of deaths was sensibly diminished.
CASE II.—Melser, a light mulatto boy, aged 16 years. Had been ill ten hours when I first saw him. Had had rigors; at the time of seeing him, had intense, burning fever; skin harsh, hot, and dry; face flushed, upper part of it swollen; eyes injected, red, fiery, and glassy; tongue covered with a dense white coating; pulse 115; great torpidity and prostration; could get no answer from him; very bad case; but little hope for him. Ordered mild chloride of mercury, grs. xvj; jalapa, grs. x; divide chart. 2, one immediately, to be followed, in six hours, by sulphate of magnesia, see; mustard bath, and sinapisms to extremities; cooling application to head.
2d day. Patient no better; disposed to delirium; pulse 120, thin, and easily compressible; other symptoms same as before. Repeated mustard bath, made stronger than at first; mild chloride of mercury, grs. xij; Dover's powder, grs, vj; divide chart. 10, one every hour.
3d day. All the symptoms same as yesterday; no sign of mercurial impression. Continued mercury in small doses; renewed mustard bath; allowed lemonade, pellets of ice, and cold applications to head; felt disposed to humour him, or let him alone altogether, to die in peace.
4th day. No change for the better; is slightly salivated. Determined to try the effect of a sedative dose of quinia; having first freely evacuated the primæ viæ with a full dose of the sulphate of magnesia, gave him sulphate of quinia, grs. xviij. The fever and all the violent symptoms subsided in about six hours after.
5th and 6th days. Continues free from bad symptoms; is disposed to be playful. Ordered him a small dose of sulphate of magnesia; would have given him some tonic, but suspected his employer, a tavern-keeper, of secretly dosing him with brandy.
7th day. Though feeble, he commenced to attend a little to his duties about the house; and although I called several times to see him, there was no occasion for further treatment. His youth, robust constitution, unabused by any excess or vice, and its fresh recuperative energies, no doubt all combined [24] to effect the wonderful change. With less favourable ground to work upon, the result must inevitably have been fatal.
CASE III.—Mr. P___, aged 27; a native. Saw him in the first instance of attack; had cold hands and feet, and rigors; severe pain in the frontal region, back, and knees; flushed face, and moderately injected conjunctiva; pulse 80, disappears under moderate pressure; complained of thirst and internal heat; tenderness of epigastrium, but no nausea; tongue coated white. Ordered mild chloride of mercury, grs. x; jalapa, grs. v; to be followed, in six hours, by castor oil, see; mustard bath and sinapisms to extremities; allowed ice-water, or lemonade in small quantities; made cold applications to the head. Second visit of the same day, prescribed mild chloride of mercury, in two-grain doses every half hour.
2d day. Slight abatement of symptoms; has had four small, dark, bilious evacuations from the bowels; slight diaphoresis; no trace of salivation; complains most of the head. Applied a fly-blister to the nape of the neck; continued mercury, in two-grain doses; repeated mustard pediluvia and sinapisms.
3d day. Found patient a little better; gums slightly touched with mercury. Ordered sulphate of quinia, in two grains, every hour, until twelve grains are taken; would have commenced sooner, but dreaded cerebral congestion; continued mustard baths.
4th day. Pain in lumbar region increased; complains, also, of pain in the abdomen; coating on tongue increased in thickness and density, is less white than at first; pulse 60, soft, gaseous, or rather felt as if globules of air were passing under the finger; it disappears under the slightest touch; bowels constipated; all the other symptoms seemingly better; but it is evidently a subtle, treacherous case. Ordered castor oil, see; with tinct. opii, gtt. x; mustard poultice to abdomen; pediluvia as before; continued sulphate of quinia, in one-grain doses every two hours; allowed small portions of weak chicken broth.
5th day. Conjunctiva yellow; skin, here and there, somewhat tinged; sickened at the first spoonful of broth; nausea had commenced before it was ready for him; irritability of stomach increased during the night; at the time I saw him, on the fifth day, he was greatly distressed with retching and vomiting; threw up bilious matter; no black vomit; is thoroughly salivated. Ordered a fly-blister to the epigastrium; called at the proper time, and sprinkled the denuded surface with acetate of morphia; allowed him to swallow pellets of ice; also gave the neutral mixture.
6th day. Gastric irritability abated, but not subdued; pulse 60, and without tone; passive congestion decided, and much increased since yesterday; countenance stupidly expressive of anxiety; mind torpid; is utterly devoid of interest in surrounding objects, and at intervals delirious; refuses medicine; is indifferent as to the result of his case; bowels constipated; urine scanty and high coloured; extremities cold and shriveled; skin ashy pale, or [25] cadaverous, except where suffused with yellow, which is dusky rather than clear and bright in its hue. The action of the heart was still more depressed in the afternoon of this day; capillaries stagnant; venous current, even in the larger vessels, sluggish; low muttering delirium throughout the night, with occasional stomachic spasms, and short, sudden ejections of a thin, glairy fluid, mixed with bile; great restlessness; very difficult to control his motions. Administered soup enemeta with brandy; also sulphate of quinia; repeated one or the other of these, in small quantities, at short intervals.
7th day. Collapsed state supervened; respiration oppressed, quick and short, interrupted with sighing and occasional hiccough; jactitation continued; but the patient was too far gone to exhibit the uncontrollable motions which characterized him yesterday; profound coma now ensued, and death soon closed the scene. Within an hour after death, the entire surface assumed a seep saffron hue, except the dependent parts, which exhibited extensive suggillation.
With immaterial variations, this case might stand for one-third of those which terminated fatally. It will be seen, I trust, from these three cases, and from the following one, the last which will be adduced from my own note-book, that the selections have not been made with a view to astonish the reader with the exhibition of extravagant specimens, aberrant from the normal phenomena which characterized the disease; but rather to present those which might serve to indicate the ordinary course of symptomatology and treatment. It would not have been difficult to have substituted for these, cases in which the wildest and most extraordinary symptoms occurred; but as they were the exception and not the rule, the time would have been spent in vain, so far as a correct transcript of the disease is concerned.
CASE IV.—Mr. J___, aged 45 years; a native. Saw the patient in the first instance of attack; had excessive rigors, or rather chills; he trembled sufficiently at intervals to shake the bed; severe pain in head, back, and knees; epigastrium very tender; stomach irritable, with nausea and occasional retching and vomiting; eyes injected, red, and watery; face much flushed; conjunctiva and skin tinged with yellow; pulse 90, somewhat full and round, but soft, and disappears under slight pressure; tongue has a thick yellow coating, deeper in shade in the centre, and fading into almost white at the margins, while the tip and edges of the tongue were of a fiery red; the mouth and fauces were also remarkably red, and moist, or rather had a glairy, viscid matter adhering to them; bowels constipated; mind wandering; speech at times incoherent; spirits much depressed; anxiety strongly depicted in the countenance; extremities cold, and towards the end of the day somewhat shriveled; a strong, fetid, sickening odour pervaded the body, and diffused itself throughout the chamber. The patient was accustomed to an excessive use of alcoholic drinks; occasionally became intoxicated. Ordered the mild [26] chloride of mercury and jalapa, see grs. x; if no action within four hours, castor oil, see; mustard pediluvia and sinapisms to extremities; bladder with ice to the head. Called again in five hours; had had one copious evacuation of very dark, almost black, extremely offensive bilious matter; had also thrown off very disagreeable ingesta from the stomach, about one hour after having taken the calomel; had taken and retained the oil well, but nausea and retching had returned when the action of the cathartics commenced; ordered mustard poultice to the epigastrium, with directions to apply a fly blister, if the former proved ineffectual in allaying the gastric irritation. Called again in the evening; found the fly blister applied, and drawing powerfully; denuded a portion of the surface, and sprinkled it with a quarter of a grain of acetate of morphia; left a similar portion to be applied in the course of the night, if needed; directed acetate of lead, see; opium, gr. j; divide chart. 15, one every hour; renewed mustard baths and sinapisms to extremities.
2d day. Stomach quiet, but will not bear pressure; pains diminished, fever subsiding; pulse 60, and devoid of tone; attributed this, in part, to sedative effects of acetate of lead, and therefore discontinued it; alvine dejections almost tarry in appearance; urine very high coloured; both discharges scanty; yellow hue of skin very much deepened; restlessness increased; mind wandering; at intervals quite delirious. Ordered sulphate of quinia, see; divide chart. 10, one every hour; mild chloride of mercury, one grain every hour until its constitutional effects appeared; repeated mustard baths and sinapisms; allowed weak animal broths and iced brandy and water.
3d day. Extremities cold; strength failing; pulse 44, and very feeble; occasional spasms; spells of delirium more frequent; tenderness of epigastrium increased; stomach irritable; vomits a light-coloured fluid, containing a dusky flocculent matter; stools more frequent than before, very black and tarry. Sprinkled the still denuded epigastrium with acetate of morphia; gave effervescing draught, pellets of ice, iced brandy, and continued sulphate of quinia. In the afternoon of same day, pulse 50; the vomit less in quantity, recurs less often, but is rather more abundant in dusky flakes; ventured to renew acetate of lead; two grains every hour, until ten grains should be taken; to counteract depressing effects, combined it with opium; prepared the family for probable fatal result.
4th day. Pulse continues at 50; coating on tongue almost black; tendency to fissure; gums inflamed, tender, and swollen, look somewhat as if the mercury had made an impression, threaten to bleed; mind very torpid; occasionally exhibits wild delirium; vomiting increased; the matter ejected is now quite brown, flakes still darker, and more abundant, begins to assume the appearance of weak Mocha coffee. Ordered soup and brandy, and soup and quinia injections. No other treatment this day; felt disposed to leave him without further effort to save him.
5th day. Had passed a fearful night; delirium had become wild and un- [27] controllable; disturbed the neighbourhood with outcries and ravings; had fainted once during the night; vomit very black and copious, one while issuing with much straining, then in forcible jets or columns, seemingly without effort; found the patient in the morning with cold, clammy, disagreeable skin; collapsed, unconscious; the material of the vomit nearly exhausted; the peculiar, fetid, sickening odour present; tremors and convulsive movements agitated the frame, with occasional shudderings; patient almost pulseless; respiration laborious; profound lethargy now ensued, and exhausted nature yielded the unequal contest in the afternoon of this day.
The fifth day was especially fatal. It was particularly dreaded both by the patients and their friends. In many cases, nothing could remove their trepidation until it had passed. During one period of the epidemic, this day was scarcely less the cause of panic than the disease itself. The intemperate and broken in constitution fell in from thirty to seventy hours, and may have numbered fifteen per cent. of the deaths; but the number of deaths on the fifth day could not have been fewer than thirty per cent. The seventh was the day of next greatest mortality. Those who survived the ninth day, generally recovered. Or, if they died after that day, it was chiefly through imprudence, relapse, too sudden change of air, or of some of the numerous sequences entailed by the disease. Thirty-five per cent. of the deaths were characterized by black vomit, either in its partial or full development. The case just cited, though not the most intense instance which can be adduced, affords a very accurate exhibition of the vomit in its milder as well as more severe aspect.
The following cases have been kindly furnished by my friend Dr. J. M. Covert, late of Charleston, S. C., now of Portsmouth. They exhibit some variations from thos already given, and include one of recovery from supposed suppression of urine.
CASE V.—September 1. Called to see Miss ___, aged 15 years. Sanguine temperament; exceedingly nervous; pulse 98; tongue covered with white thick fur, edges intensely red; eyes suffused, and capillaries congested; urine highly coloured and scanty; severe pain over the supra-orbital ridge; weariness in limbs, and lancinating shoots of pain in the back; nausea. Ordered mustard pediluvia; ice to head; patient to be wrapped in blankets; no fluids to be taken; allowed pellets of ice in the mouth to assuage thirst; administered sulphate of quinia; sub mur. hydrarg. see grs. x; to be followed at night by castor oil.
Sept. 2. Bilious emesis; skin hot and parched; tongue more foul than preceding day; had operated freely; bilious dejections; pain intense in head; slightly delirious; excessive thirst; urine as before. Repeated foot-bath; administered sulph. quinia; sub mur. hyd. see grs. viij; ft. pil. 4; one every two hours.
3d. Sent for at daybreak; called in a consulting physician. Patient wildly delirious; excessive epistaxis; pulse 100; had three operations, watery; tongue [28] still foul; nausea continues; restless, tossing from side to side. Ordered fly blister to nape of neck, ice to forehead, blister to epigastrium; administered sulph. morph. gr. j; bicarb. sodæ see; aqua see; one tablespoonful every two hours.
4th. Pulse 90; epistaxis less; delirium slight; passed a restless night; some nausea; no operation since preceding day; looks haggard and careworn; tongue crisp, red, and furrowed, with a tendency to bleed. Continued the mixture; poultice to blistered surface; enema of soup.
5th. Epistaxis ceased; slight nausea; pulse 78, small and feeble; tongue cracked and, with the gums, bleeding; feels a trifle better, but very weak. Ordered dilute mur. tinct. ferri to gums; sulph. quinia, grs. viij; elixir vitriol q. s.; syr. zingiber. see; tablespoonful every two hours.
6th. Pulse 80; tongue dry, and brown in centre; gums sore, bleeding ceased; feels much better; asks for food; allowed chicken soup, soft boiled egg. Ordered sub mur. hyd. grs. vj, in one-grain doses as an alterative. Continued sulph. quinia mixture.
7th. Pulse 82; made an effort to rise, but found strength wanting; tongue clean and pleasant. Ordered soup, and chicken, and wine.
8th. Pulse 84; patient sitting up in bed; has good spirits; craving appetite for pickles. Allowed lemonade, chicken soup, and eggs.
9th. Feels exceedingly well, and convalesced rapidly.
CASE VI.—September 6. Mrs. P___, aged 26 years; delicate frame, nervous temperament. Taken with severe chills, followed by fever; nausea; headache; pain in limbs and back; tongue white and flabby; eyes suffused; pulse 96. Ordered quinia and calomel, and oil at night; sinapised pediluvia; ice to head.
7th. Patient exceedingly feeble; constant nausea and vomiting; anorexia; pain in head intense; tongue flabby and foul; had two operations, bilious; pulse 106; urine copious; capillaries dull on pressure. Ordered blister to epigastrium, and mustard to dorsal spine; effervescing draught; morphia at night; cold applications to head.
8th. Patient almost comatose; pulse too feeble and quick to be counted; disappears under touch; excessive vomiting; matter slimy; scarcely answers when spoken to; tongue as before, and slightly red at the edges. Directed warm poultice to blistered surface; creasote see xx; sulph. ether, spr. lavender, see see; a teaspoonful every half hour.
9th. Sent for early in the morning; patient almost gone; pulse and tongue as before; eyes fixed and glassy; respiration hurried and feeble. Gave brandy and chloric ether; soup enemata every hour, containing a spoonful of brandy.
10th. Patient about the same; stomach refuses to take anything. Repeated the treatment of yesterday; reapplied fly blister; continued the creasote mixed.
[29] 11th. Is slightly better, but very feeble. Ordered champagne, and repeated soup enemeta; morphine and soda mixture at night.
12th. Improving very slowly. Continued treatment—enemata, stimulants, and chicken soup.
17th. Is convalescent; able to sit up in a chair.
20th. Patient doing so well that visits were discontinued.
CASE VII.—September 10. Miss ___, aged 19 years. Fever high; pulse full and bounding; eyes watery; tongue thickly furred, yellow; urine scanty; great disposition to sleep; no nausea. Ordered foot-bath; gave effervescing draught every two hours.
11th. Fever increased; pulse 102; eyes dull; tongue slightly cleaned; had several operations; disposition to sleep the same; complains of no pain; answers carelessly. Continued treatment of yesterday.
12th. Found patient asleep; aroused her with difficulty; pulse less frequent and weaker; tongue cleaner; slept the whole day; eyes very dull; whole appearance tranquil. Ordered sulph. quinia mixture; allowed tea and toast at night.
13th. Patient, as usual, sleepy; would answer no questions; pulse 90; fever abated; on inquiry, was told she had passed no urine since the previous evening. Ordered spr. acetat. ammon. and turpentine mixture. Called at night to pass the catheter, in hopes that it was merely retention of urine, and not suppression; passed it at four different times, but no urine flowed; regarded the case as hopeless; told the parents so; consulting physician corroborated my statement.
14th. Was sent for, and told that the patient had passed about a gill of urine, at 10 o'clock A. M., after an interval of about thirty hours. Immediately ordered water-melon seed tea, and drinks ad libitum.
16th. Patient entirely recovered.
In concluding this brief account of the treatment which obtained in the late epidemic, I feel constrained to say that the only effectual means of safety from the ravages of yellow fever are—not in medicine, but in HYGIENE. The ounce preventive is here emphatically of more value than the entire pharmacopœia. Remove the known causes; leave nothing for the peculiar, unknown poison to act upon, and epidemic yellow fever is simply an impossibility. I confess, however, that in some localities, this would be more than an Augean task. The only remedy, in such instances, is absolute abandonment of the locality. (1) I have broached the subject of the inadequacy or remedial
The burning of tar in the public street has been extensively practiced in various places during the prevalence of epidemic yellow fever. This seems to me absurd. If tar be a preventive agent, or even a purifier of the air from the poison of this disease, why are not sailors, who see tar, feel tar, taste tar, smell tar, burn tar, live in tar, and are smeared with it from their tarpaulins to the soles of their shoes, exempt?
[31] measures to cure the disease for another reason besides its intrinsic truthfulness. Practitioners, from every section of the country, some of them perhaps with but little experience, assemble at any given infected locality. They arrive, each with his peculiar preconceived ideas, and with the full determination to excel all competitors by his heroic performances. The result is, over-treatment. And it is only after the death of three in every four of his patients that the inexperienced practitioner allows more moderate councils to prevail, and expects less from remedies. To alleviate and control was the aim of the wisest and most skilful; and such was the treatment under which the greater proportion of the survivors recovered.It is subject of regret that there was little opportunity for post-mortem examinations in this epidemic—at least in Portsmouth. Two causes militated against them. No city hospital was established at this place; in consequence, no doubt, of the humane action of the United States Government, which opened the wards of the Naval Hospital established there. The medical corps of this admirably constituted establishment offered me every facility for making autopsies upon its legitimate inmates of the naval service; but, from obvious reasons, not upon the bodies of deceased citizens. This narrowed down the opportunity to a very small scope, owing to the skill and admirable medical police there. I visited the hospital daily, watchful of every case that was likely to terminate fatally, but without the desired success. Two or three partial autopsies were made by the medical corps of the institution, but, from whatever cause, my request to include an account of them in this essay has not been acceded to. On the other hand, in addition to the natural repugnance to it of the families in town, this sickness inspired such terror that the bodies were often coffined and hurried off to interment while yet scarcely cold, entirely precluding the possibility of making the desired examinations. But one post-mortem was made in Portsmouth; of this there is no satisfactory account. Norfolk, from the facilities which its two temporary hospitals afforded, was much more favoured in this particular than the former city; and it may be that some important statements may yet see the light through the agency of those concerned in the investigations there made. But the epidemic at New Orleans, in 1853, and that at Norfolk and Portsmouth, in 1855, are acknowledged to be of the same type, as well as of similar virulence. Through the kindness of my friend, Dr. Hewit, of New York, I have been furnished with a series of post-mortems, made during the former epidemic by Dr. Vaude. They have never until now been published, and they will, at least in some measure, serve to fill up the hiatus in this branch of my subject. It might be regarded as a drawback to their utility, that the symptoms which marked the course of the disease, in each particular case, are not also recorded. These, however, may, in the main, be readily inferred by the lesions exhibited in the subjects.
[31] CASE I.—Boy, aged 13; complexion pale. Extensive dermic post-mortem congestion; rigor mortis slight; congestion tinged yellow. Heart full of dark blood; no coagula. Lungs excessively congested. Liver normal in consistence, coffee-ground colour; vessels congested. Gall-bladder contained an ounce and a half of dark-green viscid bile. Bladder empty. Spleen more tough than natural. Kidneys congested.
Head.—Scalp dry; dura mater dry; longitudinal sinus full of blood. Serum effused beneath the arachnoid; this membrane opaque; capillaries congested throughout, though firm. Abdomen.—Mesenteric gland enlarged. Stomach containing a pale acid fluid; mucous membrane thickened, softened; mucous membrane of the colon thickened, intensely congested, softened.
CASE II.—German woman, aged 30 years; moderately fat; three hours after death. Had been sick seven days; admitted day before; no treatment. Colour yellow; lungs intensely congested. Heart containing coagula; valves yellow. Liver dark red, intensely congested; gall-bladder containing see dark-green viscid bile. Stomach containing black vomit, acid; mucous membrane hypertrophied, firm, congested. Mesenteric glands enlarged. Mucous lining of alimentary canal congested. Bladder contained a small quantity of acid, albuminous urine. Uterus congested, containing a coagulum. Head.—Dura mater congested; serum effused beneath arachnoid; this membrane opaque; the substance of the entire brain intensely congested and soft.
CASE III.—Man, aged 35; twelve hours after death. Yellow dermic post-mortem congestion; lungs congested, partly post-mortem. Heart containing coagula, valves yellow. Liver congested, softened. Spleen enlarged, engorged. Stomach containing black vomit, acid; mucous membrane pale, firm. Urine acid, albuminous. Head.—Serous effusion beneath arachnoid. Brain congested and softened throughout. Kidneys deep red, engorged.
CASE V.—Man, aged 35 years; twelve hours. Skin yellow. Lungs empty. Heart empty. Liver congested; colour of internal surface olive-green. Gall-bladder containing an see of green, viscid bile. Stomach empty; mucous membrane congested, softened; mucous acid. Blood acid, and coagulating firmly. Colon and rectum filled with coagulated blood. Mucous membrane of entire track of bowels congested, softened. Head.—Dura mater yellow; sinuses empty; serous effusion beneath arachnoid; brain intensely congested throughout its substance. Urine acid.
Having displayed, with as much clearness as the material in hand permitted, the chief characteristics of the late epidemic, it seems proper to note the sanitary lessons it is calculated to teach. If there be any means by which Norfolk and Portsmouth, or any other place obnoxious to the disease, may avert its inroads, they ought to be at once applied. I have expressed it as my decided conviction, that the proper, and only possible means of preventing [32] the terrible ravages of yellow fever, is a strict hygienic system. I use the term in its broadest acceptation, including not merely those objects which are used by man and have a bearing upon his health, but also whatever in any manner relates to the preservation of cleanliness and the purity of the atmosphere. So far as Portsmouth is concerned, it would be extremely difficult, if not impossible, to obviate some of the conditions which militate against good health. The low plateau on which it stands, and water being everywhere abundant a few feet below the surface of the ground, preclude the possibility of proper drainage. There being therefore no receptacle for the waste, offensive waters of the city, it lies in pools, festers, and slowly evaporates, and of course forms one item of contamination of the surrounding atmosphere. Add to this the offal, garbage, and every species of effete matter inseparable from cities and towns, and hourly augmenting, and the difficulties in the way of improving the hygiene, in these particulars, seem sufficiently appalling. Norfolk, as before remarked, has somewhat the advantage of her sister city in these particulars. It rises gently as it recedes from the river, and is susceptible of much improvement in the matter now under consideration, and ought, without delay, to set about the construction of sewers adequate to the complete drainage of the city. But is there no feasible plan to effect the same end in Portsmouth? I believe there is. In all well-regulated cities it is the custom, on stated days of every week, to send to each house, carts, to collect refuse matter, and dispose of it. Portsmouth might adopt this system, and expand it so as to include all refuse water. Let it be enacted by law, that no person shall throw into the public highways, or private lots or yards, or in any other place within the city limits, any garbage, or animal or vegetable matter whatsoever; or any waste water, or fluid of any kind; but shall preserve it in a convenient vessel until the carts provided by the city call and remove it; and let it be the duty of those appointed to collect it, to empty it into the river at a convenient distance from the city. By these means one source of noxious vapours may be effectually disposed of.
Another important step would be to fill up the marshes and small creeks within the city limits. This would be certainly a more formidable task than the former; but nevertheless is equally capable of accomplishment. Art overcomes many of the inconveniences of nature. Rocks, hills, and mountains are laid low, and the valleys are exalted before the steady march of human improvement. But as there are no hills within eighty miles of Norfolk and Portsmouth, whence can materials be procured for the performance of the task suggested? From the sea-shore, in the immediate vicinity of both cities. Let suitable vessels at proper times be constantly employed in the conveyance of sand, and deposition of it upon the spots indicated. Let neither time nor money be taken into consideration in this work. The season of the year alone should be considered. The work should not proceed during the spring or summer months, since experience proves that the mere upturning of the [33] earth has been productive of epidemic yellow fever; but all the remainder of the year should be employed in it. As a proof of the feasibility of such a task, if any doubt, I would state that material enough, within a short time past, has been removed from the northern section of Manhattan Island, and from the northwestern part of Philadelphia, to fill up the spaces referred to, six times over. And, as an inducement to accomplish the task, I would add, that since Dock Creek, Philadelphia, has been annihilated in this way, no yellow fever has originated or prevailed in that locality. Even during the epidemic of 1820, not one case occurred on Dock Street; although it approached to within a square on one side, and less near on all its other points. I have named the sands of the sea-shore as the proper material, because it is quite as easily obtained as the dredgings of the river lying between the two cities; and the latter being of rich mould, generally composed of organic matter, is of itself pestiferous. Should the task be accomplished, another inexhaustible source of noxious vapour would be forever destroyed; and what would be only second in importance to this, the numerous wooden bridges, and that still more obnoxious mass of decayed wood, the causey connecting Gosport with Portsmouth, would disappear. And still further, those other masses of decaying vegetable matter, in the shape of rotten logs, and crumbling hulls of vessels, which are laid up on this fermenting plain of mud and filth (to say nothing of its successive crops of slimy vegetation) would all vanish; and these other sources of epidemic disease be also removed.
As a third measure towards a correct hygiene, I would advise the filling up of certain well-known offensive docks, which have long been the pestiferous and death-bearing agents to all whose poverty or avocation obliges them to reside in or frequent their vicinity. And together with them the total destruction of all those filthy, old, dilapidated, tottering tenements which disfigure the fronts of both cities. Water will not cleanse them; human skill cannot repair them; nothing short of utter annihilation will be fully adequate to their effectual removal as seats and centres of epidemic disease. And in providing other places of residence for those who occupy those miserable abodes, care should be taken not to permit too many persons to reside in one house; and further, the tenants should be obliged to observe the rules of cleanliness, both of person and property.
The last, and at the same time one of the most important of these suggestions, relates to the remains of the sacred dead. They can scarcely be said to rest beneath the sod. They lie in tiers; and some of them, from the sad necessity of the case, uncoffined; while but thin strata of sabulous earth separate them from the water below and from the superincumbent air. The average depth of the graves is about four feet—the deepest five; and in many of them three bodies are placed one upon the other. When the summer's sun shall pour its fervid rays down upon this decaying mass, can it be otherwise than that their noxious gases will commingle with the purer air, and sooner or later aid in reproducing other harvests of disease and death. Here are heat, [34] moisture, animal and vegetable matter, in one putrescent mass; and, if infection anywhere exists, must in this mass abound. But, again, in two cities having a combined population of twenty-seven thousand people, how many domestic animals must die annually, whose bodies are hastily and carelessly disposed of? Enough, certainly, to add a very sensible proportion to the many other sources of deleterious air. I am aware that it is affirmed by some that animal decomposing matter is not deleterious. This is far from being established by sufficient facts. But suppose it were so established; I am not speaking of animal decomposition alone; but this, combined with other elements, which, all agree, concur with an unknown mephitic agent in the production of yellow fever; and especially am I speaking of that animal decomposition—the deceased by the disease—in which, if such agent exist at all, it must be copiously treasured up until circumstances combine to redevelop its virulence. What, then, is the remedy here indicated? It is the disinterment of the dead, and their removal to a distance of not less than five miles from either city. It is the total annihilation of intermural, or even near by suburban cemeteries—here or elsewhere. It is to forbid, by legal enactment, any person from leaving exposed, or burying within five miles of either city, the body of any animal whatsoever.
These four are the principal works whose accomplishment is absolutely necessary to the future healthfulness and well-being of Norfolk and Portsmouth; and if they, or their equivalent, are not accomplished, it is unquestionable that sporadic and, at intervals, epidemic yellow fever will continue to repeat its ravages, and heap its hecatombs of human victims upon those whom it has already slain. I have not pressed the point of the minor hygienic rules—cleanliness of house, of person, of lots, of out-houses; the renovation of property within and without; destruction of infected clothing and bedding, or at least the thorough disinfection of them; the abandonment of basements and cellars as places of residence, and many other matters of like import, because these are all either included in the above or will readily present themselves as objects of consideration; and any evils that might arise from a neglect of them must, in many instances, have been already prevented by the appropriate remedies.
The only objection which can reasonably be brought against the measures here suggested is the cost. This is unquestionably an important consideration. Scarcely any community in time of health is willing to pay extensively for those works which, in the midst of an epidemic, all agree should have been performed. The outlay necessary for the accomplishment of them cannot but be considerable. But would any outlay be too great in view of the benefits to be derived from them? A glance at the comparative cost of the improvements on the one hand, and of such an epidemic as that of Virginia, on the other, will be a sufficiently emphatic response. The loss sustained by any community from such an epidemic far exceeds the cost of even greater works of improvement. The estimates which I here venture to present, being [35] based upon observations rather than actual statistical tables, assume to be but approximations; but I will endeavour to fall short, in making them, rather than exceed the actual expense. From certain works which have fallen under my observation, I suppose that one million of dollars would cover the entire expenditure of filling up the runs, swamps, and offensive docks in both cities. For the sake of margin, call it two millions. The known cost of disinterring bodies and replacing them in other ground is six dollars each. For the sake of margin, again, say ten. Estimating the number in all the cemeteries there to be thirty thousand, the entire cost of the transfer would not exceed three hundred thousand. In the third place, the cost of removing garbage, waste water, and all offensive fluids—supposing twenty men and horses at twelve dollars each per week—would be two hundred and forty thousand dollars per annum; or, making the estimate for five years, one million two hundred thousand dollars. This would give a grand total of three millions and five hundred thousand dollars as the entire expense for the accomplishment of all these works. Contrast this with the loss resulting to both cities from one such epidemic as that which has just desolated them. It would be impossible to estimate the entire loss which a community must sustain under such circumstances, in diverting business from the ordinary channels altogether, or during the sickly season, and of many who will seek other domicils in preference to those liable to such fearful invasions; but it is known that there are now missing from the two cities four thousand persons, who resided there before the late epidemic commenced. It would be an exceedingly low estimate to say that the average advantage to any community of each member of it is five hundred dollars per annum. For, though children and invalids are non-producers, they are consumers; and, on the other hand, many are worth to the community from one to ten thousand dollars, or more, according to their position or business. But, taking it at the lowest estimate, the actual loss per annum to both cities by the late sickness is two millions of dollars; or, making the estimate as before, for five years, it would be ten millions, nearly three times the cost of the improvements. But the average of human life is thirty-three years. The actual loss, therefore, is sixty-six millions; all of which could be saved at an outlay of less than four millions. In these estimates, the main consideration has been thrown aside—namely, the preservation of human life. In view of this, I would ask, what sum should be considered great?
There is one question which, before closing this essay, I feel it incumbent upon me to ask. Have Baltimore, Philadelphia, and New York no reason to fear the inroads of epidemic yellow fever? The movements of epidemic disease are mysterious, and, as yet, remain inclosed in the secret councils of the Most High. It pleases Him to allow, at times, our inquisitive nature to unlock the storehouse of the laws by which He governs the material objects interesting to man. But this has not yet been permitted either as to the causes or the nature of the epidemic influence. At one time it seems com- [36] paratively to slumber; at another, it starts forth from some given point, and ceases not until it has encircled the globe. Such was the case a few years ago with cholera asphyxia. Such, within certain limits, has been the habit of the plague, and of many other diseases; and such, also, is the history of yellow fever. It has made its appearance on the Atlantic coast as far north as Quebec; and all our Atlantic cities have more or less experienced the deadly influence of its presence. This is especially true of Philadelphia, and though many of the predisposing, or at least inviting, causes do not now exist here to nearly the same extent as they formerly did, yet the late quasi epidemic of 1858, in which there were one hundred and seventy cases, of whom one hundred and twenty-eight died, admonishes us that we are not secure from invasion. It is a peculiarly malignant type of the disease which now prevails upon our seaboard. Whether its line of travel be certainly and inflexibly northward, I shall not take it upon me to affirm; but does it not seem so to be? First we have an outburst of its violence—not an ordinary visitation—in 1853 at New Orleans, which aroused the sympathies of our entire people. Next, the same fearful type prevails to a like extent in 1854 at Savannah and Charleston, not to speak of other intermediate places which have for the first time been brought by it into undesired notoriety; and now, in 1855, with almost unprecedented violence, at Norfolk and Portsmouth. I believe that Baltimore, Philadelphia, and New York have grave cause to look in time to their narrow courts and lanes; their filthy, ill-ventilated, overcrowded tenements; their pools, ponds, runs, creeks, marshes, docks, common-sewers, slaughter-houses, offensive manufactories, privies, disposal of garbage, and other public and private nuisances; which, if not so many salient points of epidemic disease, are factors of the morbific agent when blended with their exhalations. Should those whose duty it is to attend to these matters neglect it until the enemy makes its fatal onset, when it defies a hygiene too late applied, what appalling horror must ensue; and what excuse can be rendered to the families of the slaughtered hosts who would fall by their neglect? They are duties which should be performed under any circumstances; how much more when such an enemy is hovering on our coasts!
While it is subject of universal acknowledgment that—in Philadelphia, for example—many of those conditions which are more or less connected with morbific influences in general, and this of yellow fever in particular, have been diminished; that streets have been properly graded; runs, and creeks, and marshes either filled up or converted into well-constructed culverts, and covered over with earth; that frame tenements, with their masses of decayed wood, have been forbidden by law; that means of free ablution have been multiplied; and many other salutary works of a good hygienic police have been inaugurated; nevertheless, much pertaining to a healthful regime still remains unaccomplished. Perhaps, too, it is not sufficiently noted that while the present supply of water was ample fifteen years ago, that the increase of population, and especially of the poorer classes, which most need [37] multiplied facilities and encouragement in its use, have so outstripped the provision made for them that, in certain localities, it is with difficulty that water can be procured for ordinary household use; and so feeble is the stream which issues from many hydrants that, if two neighbours desire to draw water at the same time, one party is obliged to wait until the other is accommodated. In certain of the higher localities, the water does not run from them at all from one and a half to two days of every week. In other places there are no hydrants whatever. Whereas the supply ought to be so abundant that not only there might be no interruption to a full flow, and every poorest person might have his bath-house, and every court, lane, and alley smell as sweetly as a spring-house, but so that fountains might have force and liberty to play in every public square and private garden; while streams of pure water should have leave to run continuously along every gutter and through every common-sewer. Thousands of dollars are annually wasted in every community, which, if properly applied in this manner for the benefit of the citizens, would enable every community on the Atlantic coast to laugh, at least at telluric and malarial epidemic disease.
Let us view the subject from another point of view. And although, for the convenience of illustration, I make Philadelphia the occasion of my remarks, by a simple substitution of name they will be found equally suitable to many of our seaboard towns. We rest in fancied security from the inroads of epidemic yellow fever. Why? Because, omitting the slight threat of 1853, only the oldest inhabitant can say, I have seen such a phenomenon. There has been no epidemic visitation here since 1820, a period of thirty-five years, or before the present generation was born; there it cannot again occur. This fallacious hope would have been poor consolation when, on one occasion, it, being absent for forty-two years, returned in 1741 with avenging force; and when, again, after an absence of thirty-one years, it recommenced its ravages in 1793. (1) A protracted withdrawal, therefore of its unwelcome presence is no ground of security against its return. Cleanliness and a perfect freedom from inviting causes are the only well-founded bases of hope against it. Dr. R. La Roche, in his voluminous digest on this subject, has well expressed the true grounds of apprehension of its return. He says: "Morbid influences which, in other cities or regions, subject the residents and visitors to febrile diseases, and especially to that form of them which constitutes the main object of our inquiries, exist in our midst. They depend on the natural, uneven, and irregular condition of the city plot; on the vicinage of the river side; the peculiar quality, natural and artificial, of the soil, in many parts at least of its surface; the compact construction of the houses, and the narrowness, imperfect ventilation, and filthiness of the streets in certain sections of the city. They arise also from the numerous courts and
(1) The periods at which yellow fever has successively invaded Philadelphia as an epidemic, are 1699, 1741, 1747, 1762, 1793, 1794, 1797, 1798, 1799, 1802, 1803, 1805, 1820, and slightly in 1853.
[38] alleys, many of which are closed at one end, unprovided with a sufficiency of water, imperfectly drained, often unpaved (damp cellars), to say nothing of the piggeries (cow-sheds) and other nuisances they contain; the denseness and squalid character of the population of these localities; the defective mode of construction, and the physical peculiarities of wharves, built of perishable timber, and filled up with animal and vegetable remains and rubbish of various kinds; as well as from the condition of the docks and the proximity of the shipping. Objectionable localities—though more numerous, perhaps, formerly than they are at present—may be found in almost every district, even in the very heart of the city, but abound more in some portions of it than others." (1) The Sanitary Committee of the Board of Health have also recently given, in an official report, a graphic description of the prevalence of incentive causes to epidemic disease. They restrict their account to "a limited district," but it can with certainty be applied to several districts both of this and the other cities included under this account. The Committee says: "It should not be overlooked that there exists a limited district in one of our suburbs, a locality that is abundantly fruitful in originating or propugating disease; and where at all seasons, winter and summer, spring and autumn, we anticipate its eruption in some frightful or protean form. In this almost isolated neighbourhood we find an excess of a vagrant population, half fed and half clothed, crowded together in almost untenantable houses, and in open and humid cellars, located in narrow streets and narrow alleys, and pent-up courts, badly ventilated and badly lighted. In this forbidding district, we could enumerate many fruitful causes for disease operation upon the half famished and bloated bodies of a depraved and mixed population, whose constitutions have been undermined through the ravages of intemperance and exposure, the accumulation of filth, and impure food and air, accompanied by the far more ruinous effects of a life of moral shame and degradation, become the fit receptacles, and afford the materials for the growth and reproduction of those morbific agents which constitute disease." (2)
(1) La Roche on Yellow Fever, vol. i, pp. 31-2.
(2) Report on joint committee, p. 36.
With these agents existing and at work in all our seaboard, what immunity can be expected from invasion should the obnoxious conditions all combine at the right moment for the production of epidemic disease; and who, in all our coasts, shall say this shall not be during the present year or the next? Like causes produce like effects, is a trite platitude, but also a truism under the force of which many a heart has been made sad and many a house desolate.From time immemorial outbursts of yellow fever have been simultaneous with the arrival of vessels freighted with disease and death. And however those, through whose oversight such mishaps occur, may shield themselves from censure by denying the facts, repeated experience declares the period [39] and the place of their arrival to be that at which the first cases of the disease occur. The commencement of the disease was thus connected in all the West India islands. In 1692, the disease for the first time appeared in Boston simultaneously with the arrival of the fleet of Sir Wm. Phipps, which had contracted it in the West Indies. In 1699, it began its ravages on the arrival of some passengers in the early part of June. In 1702, an epidemic at New York was attributed to a ship from the island of St. Thomas. In 1844, this city had another visitation, which was charged to a similar arrival from the West Indies. The College of Physicians unanimously attributed the great epidemic at Philadelphia in 1793 to importation by some vessels from the same islands, and they instance the fact of its frequent origin through these means in various parts of North America. And finally, not to dwell upon the numerous successive instances of its connection, or simultaneous outbursts, with the arrival of vessels from diseased ports, the barque Mandarin and the steamer Benjamin Franklin bear the blame, whether justly or not, for bringing it, in the first instance, into Philadelphia in 1853, and, in the second, into Portsmouth in 1855. In every instance the peculiar poison of yellow fever found the corresponding elements ready for action; and should these again concur in any given place, nothing will save the inhabitants from this most deadly pest, The question, then, is not for how long a period an epidemic may have discontinued its ravages, but what is the hygienic condition of each particular city or town. Let the boards of health, then; let the various medical bodies individually and collectively; let our city councils, and all in authority; let our police, and let every private citizen, in all our seaboard towns, as far north at least as Boston, see to it now that their cities are in a cleanly condition; that they have plentiful supplies of water appropriately used; that all nuisances are removed; that all offensive manufactories either abate the offence or be transferred into the rural districts; that ponds, marshes, pools of stagnant water, sinks, common-sewers, docks, privies, closely built courts, garbage, dead animal bodies—in a word, everything which can by any possibility provoke, aid, or abet epidemic disease, be thoroughly and entirely removed, or otherwise remedied. We may then, and only then, confidently expect a continued immunity from epidemic yellow fever; and this, whether the theory of importation or of local origin be the true one.
(The End.)
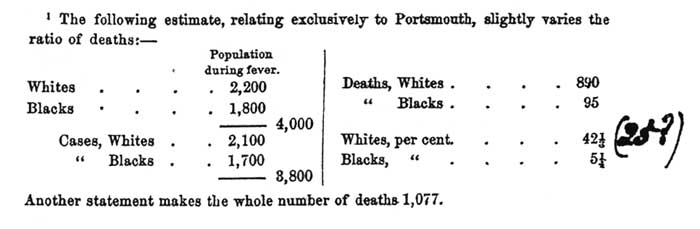
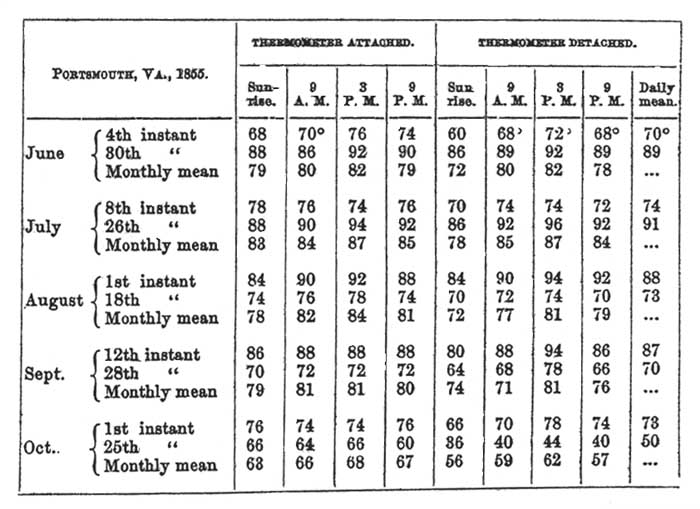
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}